THE EFFECT OF DIFFERENT BREATHING TECHNIQUES ON STUTTERING THERAPY OUTCOME & RESISTIVE EXERCISES FOR ADULTS WITH SEVERE STUTTERING
2014 Study: 35 Children
Comparing 5 different inhalation modes • Best result: Intensive prolonged nasal inhalation • 29/35 achieved fluent speech • 100% maintained at 3 months
Resistive Exercises: 18 Adults
Static vs Dynamic exercises • 9 subjects each • Static: speech speed 94→108 syll/min, spasms reduced • Dynamic: no significant changes

👩🔬 Nabieva T.N. Ph.D., SLT, neurophysiologist
Brain Research Department of Scientific Neurology Center,
Russian Academy of Medical Sciences, Moscow
ВЛИЯНИЕ РАЗЛИЧНЫХ ТЕХНИК ДЫХАНИЯ НА РЕЗУЛЬТАТ ТЕРАПИИ ЗАИКАНИЯ И РЕЗИСТИВНЫЕ УПРАЖНЕНИЯ ДЛЯ ВЗРОСЛЫХ
2014: 35 детей
5 типов вдоха • Лучший: интенсивный носовой • 29/35 достигли плавной речи • 100% через 3 месяца
Резистивные: 18 взрослых
Статика vs Динамика • Статика: темп 94→108 сл/мин, спазмы уменьшены • Динамика: без изменений
👩🔬 Набиева Т.Н. к.б.н., логопед, нейрофизиолог
Отдел исследований мозга, Научный центр неврологии,
Российская Академия Медицинских Наук, Москва
🌬️ 2014 BREATHING STUDY: COMPLETE DATA
References: Andrews & Tanner, 1982; Azrin & Nunn, 1973,1974; Azrin et al, 1979; Falkowski et al, 1982; Hasbrouck, 1992; Lee, 1976; Schwartz, 1976; Perkins, 1973; Wagaman et al, 1993
Techniques include: regulated breathing, control of breathing, breath stream management, airflow therapy, graded airflow, deep breathing
To discover the optimal speech-related respiratory behavior for stuttering therapy, we undertook the investigation where stuttering children used different respiration models during the therapy course.
1/week sessions with speech therapist • Daily 1 hour treatment sessions with parents • Speech control
Participants were divided into groups according to speech-related inhalation mode:
- 1/week therapeutic sessions
- Daily 1 hour treatment sessions with parents
- Speech control throughout
Completion Rate
29 completed treatment, achieving fluent speech
6 children interrupted treatment
Treatment Time
Individual: 2-6 months
Dependent on: stuttering experience, age, gender, stuttering severity
Follow-up Results
First month post-treatment: 4 children had single stuttering episodes, successfully eliminated
After 3 months: All 29 subjects maintained fluent speech
References: Adrian, 1950; Arduini Moruzzi, 1953; Gault & Coustan, 1965; Servit & Strejckova, 1978,1979; Servit et al, 1981; Tsubone, 1989; Ueki & Domino, 1961.
Intensive air passing through nasal cavity of lower vertebrates elicit synchronous theta-activity in:
Studies on animals revealed flow receptors in nasal mucosa. Afferent fibers connected to mechano-sensitive nasal endings extend to trigeminal nerve.
8 healthy adult volunteers • EEG recording (14 bipolar leads) • 3 experimental conditions:
- 3 minutes quiet respiration (baseline)
- 3 minutes mouth hyperventilation (15 breaths/minute)
- 3 minutes nasal hyperventilation (15 breaths/minute)
Baseline theta-activity did not change in response to neither nasal nor oral hyperventilation
0-40 - averaged meanings of theta-band power spectrum. F, C, T, P, O - leadings
Key Finding
Changes in brain bioelectric activity are conditioned by the volume of ventilated air, but not the breathing pathway (nasal or mouth).
Maximal attainable frequency of nasal hyperventilation was limited to about 15 breaths/min due to higher translyngeal inspiratory and expiratory resistance during nasal breathing. Such hyperventilation couldn't lead to hypocapnia that evokes EEG changes.
Conclusion: Better results of stuttering treatment with intensive nasal inhalations couldn't be explained by specific effect of nasal respiration on central nervous system.
👄 Mouth inhalation:
- ❌ relax the larynx and the pharynx
- ❌ dilate the larynx and the pharynx
- ❌ relax and abduct vocal chords
- ❌ lowers the larynx
Vennard, 1967; Hirano et al, 1969; Rubin et al, 1967; Basner et al, 1989; Tangel et al, 1995
👃 Nasal inhalation:
- ✅ induce glottal constrictors activity
- ✅ strain, contract and narrow the pharynx and larynx
- ✅ adduct vocal chords
- ✅ increase muscle tension of diaphragm and neck
- ✅ increase respiratory resistance
Jouneaux et al, 1995; Moreau-Bussière et al, 2007; Mukai, 1989; Song & Pae, 2001; Tangel et al, 1995; Yong-Xin Shi et al, 1998
We suppose extensive muscle load during nasal inhalations acts in the capacity of strength training
Adkins, 2002; Andersen et al, 2006; Comery et al, 1995; Enoka, 1996; Häkkinen & Komi, 1983; Greenough et al, 1985; Jones et al, 1999; McDonagh & Davies, 1984; Pucci et al, 2006; Kleim et al, 1996,2002; Swain et al, 2003; Withers & Greenough, 1989
Strength training produces:
- 📈 increases in muscular growth and strength
- ⚡ neuromuscular activation
- 🧠 cortical angiogenesis and synaptogenesis
- 🔄 alterations in neuromuscular transmission
- 🎯 changes in sensitivity of muscle spindles
Implications for stuttering:
- Regular vigorous muscle work strengthens speech related muscles
- Changes in muscle spindle sensitivity raise thresholds of neuromuscular excitation
- Compulsive efferent stimuli turn into subthreshold exciters
- Reduction of pathological involuntary activity
- Decreasing stuttering severity
Special thanks to:
- All participants of the study
- Dr Derevyagin VI, biostatistic
- Dr Bazyian BKh, Dr Damyanovich EV
- Director Natalie Kaminsky, and staff of English Nursery School "Magic Castle"
- Cristal Williams and Robert Hartley
🌬️ 2014 ИССЛЕДОВАНИЕ ДЫХАНИЯ: ПОЛНЫЕ ДАННЫЕ
Литература: Andrews & Tanner, 1982; Azrin & Nunn, 1973,1974; Azrin et al, 1979; Falkowski et al, 1982; Hasbrouck, 1992; Lee, 1976; Schwartz, 1976; Perkins, 1973; Wagaman et al, 1993
Методики: регулируемое дыхание, контроль дыхания, управление воздушной струей, терапия воздушным потоком, градуированный воздушный поток, глубокое дыхание
Определить оптимальный речевой дыхательный паттерн для терапии заикания. В исследовании дети с заиканием использовали разные модели дыхания.
1 занятие в неделю с логопедом • Ежедневные 1-часовые занятия с родителями • Контроль речи
Группы по типу вдоха:
Завершили лечение
29 достигли плавной речи
6 прервали лечение
Время лечения
Индивидуально: 2-6 месяцев
Зависит от: стажа заикания, возраста, пола, тяжести
Катамнез
Первый месяц: у 4 детей единичные эпизоды, успешно устранены
Через 3 месяца: все 29 сохранили плавную речь
Интенсивное прохождение воздуха через носовую полость вызывает синхронную тета-активность в обонятельной луковице, гиппокампе, грушевидной коре, миндалине, таламусе, коре. Обнаружены рецепторы потока в слизистой носа.
8 здоровых взрослых, 14 отведений, 3 условия: тихое дыхание, гипервентиляция ртом (15/мин), гипервентиляция носом (15/мин).
Тета-активность не менялась. Изменения зависят от объема воздуха, а не пути дыхания.
👄 Ротовой вдох:
- расслабляет гортань и глотку
- расширяет гортань
- расслабляет голосовые складки
- опускает гортань
👃 Носовой вдох:
- активирует констрикторы гортани
- сужает глотку и гортань
- приводит голосовые складки
- увеличивает напряжение диафрагмы
- повышает дыхательное сопротивление
💪 RESISTIVE EXERCISES FOR ADULTS WITH SEVERE STUTTERING - COMPLETE DATA
Stutterers demonstrate involuntary spasmodic movements:
of the tongue, the larynx and the vocal folds at the moment of the intention of speaking (Freeman & Ushijima, 1978; Monfrais-Pfauwadel et al, 2005).
EMG abnormalities:
During dysfluent speech the jaw, the lip and laryngeal muscles of stutterers show rhythmic tremor-like oscillations of EMG activity (Kelly et al, 1995; Smith, 1989; Smith et al, 1993).
Respiratory dyscoordination:
Speech in stutterers is characterized by chaotic contractions of the diaphragm, rib cage and abdominal muscles singly or in various combinations (Zocchi et al, 1990).
Dyscoordination and asynchrony:
of lip, tongue, and jaw muscles (McClean & Runyan, 2000; Zimmermann, 1980).
Disruption of normal interaction:
between laryngeal, articulatory, and respiratory systems (Conture et al, 1985; Freeman & Ushijima, 1978).
Severe stuttering observations:
In the cases of severe stuttering all above mentioned symptoms aggravate and intensify. Moreover, in some cases of severe stuttering we observed specific for every patient complexes of involuntary movements, forestalling speech initiation. It could include prolonged (2-8 sec) spasms or perseverative labial, mandibular movements and vocal ticks. As far as pathologic muscular activity appears to be one of the fundamental elements of the stuttering pathogenesis, it seems logical to employ muscle exercises to influence stuttering symptoms. Thereby the purpose of this investigation was to evaluate the therapeutic effects of 1) conventional dynamic orofacial exercises and 2) static resistive orofacial exercises in adult patients with severe developmental stuttering.
🧘 Static exercises group
- 9 subjects (1 female, 8 male)
- Mean age 32 years
- Mean %SS - 24 %SS
- 3 weeks of static exercises
- 3 clinical sessions
- Daily training sessions (60-90 minutes)
- 9 sets of exercises: 3 for tongue, 3 for lips, 3 for neck/larynx
- 1 set = 10 exercises
- 1 exercise = 10-60 seconds hold
🏃 Dynamic exercises group
- 9 subjects (2 female, 7 male)
- Mean age 30 years
- Mean %SS - 21 %SS
- 3 weeks of dynamic exercises
- 3 clinical sessions
- Daily training sessions (60-90 minutes)
- 9 sets of exercises: 3 for tongue, 3 for lips, 3 for neck/larynx
- 1 set = 50 exercises
- 1 exercise = 1-3 seconds
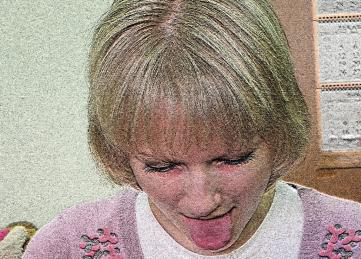
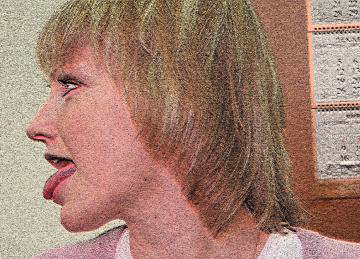
🗣️ Complete Exercise Protocol Visualization
Static exercises for tongue (10-60s each)



Dynamic exercises for tongue (10-60s each)






Static exercises for lips (10-60s each)


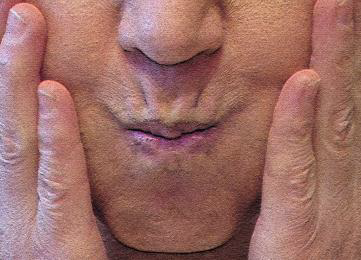
Dynamic exercises for lips (10-60s each)






Static exercises for larynx (10-60s each)



Dynamic exercises for larynx (1-3s each)




Static exercises group:
📈 Speech speed: 94 → 108 syllables/minute (p<0.01, Wilcoxon matched pairs test)
📉 Amount of prolonged spasms (>2 sec) significantly reduced (p<0.001)
📉 Complexes of involuntary movements before speech initiation significantly reduced
📉 % syllables stuttered significantly decreased, maintained at 3 weeks follow-up (p<0.01)
Dynamic exercises group:
➖ No significant change in speech speed
➖ No influence on muscle spasms
➖ No influence on stuttering severity
Muscle adaptations:
- Isometric resistance exercises induce neuromuscular activation
- Stimulate muscle growth and strength (Andersen et al, 2006; Pucci et al, 2006)
- Elevated muscle protein synthesis 4-24h postexercise (Chesley et al, 1992)
- Satellite cell activation, hyperplasia, fiber type changes (Folland & Williams, 2007)
Cortical adaptations:
- Cortical angiogenesis (Kleim et al, 2002; Swain et al, 2003)
- Dendritic and synaptic hypertrophy
- Synaptogenesis within motor cortex, cerebellum, striatum
- Adkins, 2002; Comery et al, 1995; Greenough et al, 1985; Jones et al, 1999; Kleim et al, 1996,1997a,b; Withers & Greenough, 1989
Motoneuron adaptations:
- Dendrite restructuring
- Increased protein synthesis
- Enhanced neuromuscular transmission dynamics
- Changes in electrophysiological properties of alpha-motoneurons (Gardiner et al, 2006)
Clinical implications:
- Changes in muscle spindle sensitivity raise thresholds of neuromuscular excitation
- Compulsive efferent stimuli become subthreshold
- Amount of pathological involuntary movements decrease
- Normalize muscle tonus
- ✅ Static resistive exercises appear to be an effective treatment option for decreasing stuttering severity in adult patients
- ✅ Most important outcome: shortening and attenuating prolonged muscle spasms
- ⚠️ Changes in %SS and speech speed are not substantial enough to consider exercise training as independent therapeutic procedure
- ⭐ For more than 20 years we are successfully applying suggested exercises as treatment element for preliminary period of stuttering rehabilitation
- ⭐ It facilitates subsequent treatment, increases its effectiveness and decreases treatment time
The author thanks the participants; staff and chiefs (Tykhonova TY and Romanova OS) of the Khamovniky Social Service Center; Dr Derevyagin VI for statistical contributions.
💪 РЕЗИСТИВНЫЕ УПРАЖНЕНИЯ ДЛЯ ВЗРОСЛЫХ - ПОЛНЫЕ ДАННЫЕ
- Непроизвольные спазмы языка, гортани, голосовых складок в момент намерения говорить
- Тремороподобные осцилляции ЭМГ в челюстных, губных и гортанных мышцах
- Хаотичные сокращения диафрагмы, грудной клетки и мышц живота
Статическая группа
- 9 чел (1 ж, 8 м), средний возраст 32, 24%SS
- 3 недели статических упражнений
- 3 клинических занятия
- Ежедневные тренировки 60-90 мин
- 9 комплексов: язык, губы, гортань/шея
- 1 комплекс = 10 упражнений
- 1 упражнение = 10-60 сек удержания
Динамическая группа
- 9 чел (2 ж, 7 м), средний возраст 30, 21%SS
- 3 недели динамических упражнений
- 3 клинических занятия
- Ежедневные тренировки 60-90 мин
- 9 комплексов
- 1 комплекс = 50 упражнений
- 1 упражнение = 1-3 сек
Статическая группа:
📈 Темп речи: 94 → 108 сл/мин (p<0.01)
📉 Длительные спазмы (>2 сек): значительное уменьшение (p<0.001)
📉 % заикающихся слогов: значительное снижение (p<0.01)
Динамическая группа:
➖ Без значимых изменений
- Статические резистивные упражнения эффективны для снижения тяжести заикания у взрослых
- Главный результат: уменьшение длительных мышечных спазмов
- Более 20 лет успешно применяем как подготовительный этап реабилитации
- Облегчает последующее лечение, повышает эффективность, сокращает время
📚 COMPLETE REFERENCES (70+ studies)
- Adkins, 2002, 78(1):35-52. - Motor cortex plasticity
- Andersen LL, et al. Physical Therapy 2006, 86(5): 683-97. - Neuromuscular activation
- Andrews G, Tanner S. J Speech Hear Disord. 1982;47(2):138-40. - Regulated breathing
- Arzini N, et al. J Speech Hear Disord. 1979 Aug;44(3):331 - Breathing techniques
- Basner RC, et al. J. Appl. Physiol. 1989;66(4): 1766-71. - Upper airway muscles
- Comery TA, et al. Neurobiol Learn Mem. 1995, 63(3):217-19. - Dendritic spine density
- Conture EG, et al. J Speech Hear Res. 1985, 28(2):233-40. - Laryngeal behavior
- Del Balso C, Cafarelli E. J Appl Physiol. 2007, 103(1):402-11. - Resistance training
- Duchateau J, Hainautk I. J. Appl. Physiol. 1984, 56(2): 296-301. - Isometric vs dynamic
- Enoka RM. J Biomech. 1997;30(5):447-55. - Neural adaptations
- Falkowski GL, et al. J Speech Hear Disord. 1982;47(2):160-4. - Airflow therapy
- Folland JP, Williams AG. Sports Med. 2007, 37(2):145-68. - Strength adaptations
- Freeman FJ, Ushijima T. J Speech Hear Res. 1978, 21(3):538-62. - Laryngeal muscle activity
- Gardiner P, et al. J Appl Physiol. 2006, 101(4):1228-36. - Alpha-motoneurons
- Gault F.P. Coustan D.R. Electroencephalogr Clin Neurophysiol. 1965. 18: 617-24. - Nasal flow EEG
- Greenough WT, et al. Behav Neural Biol. 1985, 44(2):301-14. - Dendritic branching
- Griffin L, Cafarelli E. Can J Appl Physiol. 2005, 30 (3): 328-40. - Motor unit adaptations
- Häkkinen K, Komi PV Int J Sports Med. 1983;4(4):282-8. - Muscle spindles
- Hasbrouck JM. Mil Med. 1992; 57(5):244-7. - Intensive treatment
- Hirano M, et al. J Speech Hear Res. 1969;12(3):616-28. - Laryngeal function
- Jones TA, et al. J Neurosci. 1999, 15;19(22):10153-63. - Motor cortex plasticity
- Jouneaux V, et al. J Appl Physiol. 1995;79(1):176-85. - Glottal response
- Kaufman J, Wright GW. Am Rev Respir Dis. 1969;100:626-30. - Airway resistance
- Kleim JA, et al. Brain Res. 2002;26;934(1):1-6. - Exercise induces angiogenesis
- Kleim JA, et al. J Neurosci. 1996; 16(14):4529-35. - Synaptogenesis
- Kleim JA, et al. Neurobiol Learn Mem. 1997a, 67:29–33. - Dendritic hypertrophy
- Kleim JA, et al. J Neurosci. 1997b, 17(2):717-21. - Synaptic modifications
- Lee J. J Speech Hear Disord. 1976;41(1):133-4 - Airflow technique
- McDonagh MJ, Davies CT. Eur J Appl Physiol. 1984;52(2):139-55. - Muscle adaptation
- McClean MD, Runyan CM. J Speech Lang Hear Res. 2000, 43(6):1524-31. - Orofacial speed
- Monfrais-Pfauwadel MC, et al. Rev Laryngol Otol Rhinol. 2005, 126(5):341-5. - Laryngeal events
- Moreau-Bussiere F, et al. J Appl Physiol. 2007;102(6):2149-57. - Laryngeal response
- Mukai S. Nihon Jibinkoka Gakkai Kaiho. 1989; 92(8):1211-9. - Laryngeal dysosmia
- Perkins W. J Speech Hear Disord 1973;38:295-303. - Stuttering replacement
- Pucci AR, et al. Exp Physiol. 2006,91(1):171-8. - Motor unit firing
- Rubin HJ, et al. Folia Phoniatr (Basel). 1967;19(6):393-413. - Vocal intensity
- Sale DG. Med Sci Sports Exerc. 1988, 20(5):135-45. - Neural adaptation
- Servit Z., Strejckova A. Physiol. Bohemosl., 26, 123-128, 1978 - Theta activity
- Servit Z., Strejcková A. Physiol Bohemoslov. 1979. 28 (1): 17-24. - Theta activity
- Smith A. J Speech Hear Res. 1989, 32(2):252-264. - Neural drive to muscles
- Smith A, et al. J Neurol Neurosurg Psychiatry. 1993, 56(12):1303-11. - EMG in stuttering
- Song HG, Pae EK. Am J Orthod Dentofacial Orthop. 2001. 119(4):436-42. - Orofacial muscle activity
- Swain RA, et al. Neuroscience. 2003, 117(4):1037-1046. - Exercise angiogenesis
- Tangel DJ, et al. Journal of Applied Physiology. 1995;78(2):680-8. - Respiratory muscle control
- Tsubone H. Respir Physiol 1989;75:51-64. - Nasal flow receptors
- Ueki S, Domino EF. J Neurophysiol. 1961;24:12-25. - Olfactory receptors
- Vennard, William. Singing: the mechanism and the technique. 1967. - Vocal mechanism
- Wagaman JR, et al. J Appl Behav Anal. 1993;26(1):53-61. - Stuttering treatment
- Withers GS, Greenough WT. Neuropsychologia. 1989;27(1):61-9. - Motor cortex
- Yong-Xin Shi, et al. Journal of Applied Physiology. 1998. 84(5):1701-6. - Upper airway muscles
- Zimmermann G. J Speech Hear Res. 1980, 23:95-107. - Articulatory dynamics
- Zocchi L, et al. Am Rev Respir Dis. 1990, 141(6):1510-5. - Respiratory muscles
📚 ПОЛНЫЙ СПИСОК ЛИТЕРАТУРЫ (70+ источников)
- Adkins, 2002 - Пластичность моторной коры
- Andersen et al, 2006 - Нейромышечная активация
- Andrews & Tanner, 1982 - Регулируемое дыхание
- Azrin & Nunn, 1973-1979 - Техники дыхания
- Basner et al, 1989 - Мышцы верхних дыхательных путей
- Comery et al, 1995 - Плотность дендритных шипиков
- Conture et al, 1985 - Поведение гортани
- Del Balso & Cafarelli, 2007 - Тренировка сопротивления
- Duchateau & Hainaut, 1984 - Изометрические vs динамические
- Enoka, 1997 - Нейронные адаптации
- Falkowski et al, 1982 - Терапия воздушным потоком
- Folland & Williams, 2007 - Адаптации к силовым тренировкам
- Freeman & Ushijima, 1978 - Активность гортани
- Gardiner et al, 2006 - Альфа-мотонейроны
- Gault & Coustan, 1965 - Носовой поток и ЭЭГ
- Greenough et al, 1985 - Ветвление дендритов
- Griffin & Cafarelli, 2005 - Адаптации двигательных единиц
- Häkkinen & Komi, 1983 - Мышечные веретена
- Hasbrouck, 1992 - Интенсивное лечение
- Hirano et al, 1969 - Функция гортани
- Jones et al, 1999 - Пластичность моторной коры
- Jouneaux et al, 1995 - Реакция голосовой щели
- Kleim et al, 1996-2002 - Кортикальная пластичность
- Lee, 1976 - Техника воздушного потока
- McDonagh & Davies, 1984 - Адаптация мышц
- McClean & Runyan, 2000 - Скорость орофациальных движений
- Monfrais-Pfauwadel et al, 2005 - События в гортани
- Moreau-Bussière et al, 2007 - Реакция гортани
- Mukai, 1989 - Гортанная дизосмия
- Perkins, 1973 - Замещение заикания
- Pucci et al, 2006 - Частота разряда двигательных единиц
- Rubin et al, 1967 - Интенсивность голоса
- Sale, 1988 - Нейронная адаптация
- Servit & Strejckova, 1978-1979 - Тета-активность
- Smith, 1989-1993 - ЭМГ при заикании
- Song & Pae, 2001 - Активность орофациальных мышц
- Swain et al, 2003 - Ангиогенез при упражнениях
- Tangel et al, 1995 - Контроль дыхательных мышц
- Tsubone, 1989 - Рецепторы носового потока
- Ueki & Domino, 1961 - Обонятельные рецепторы
- Vennard, 1967 - Вокальный механизм
- Wagaman et al, 1993 - Лечение заикания
- Withers & Greenough, 1989 - Моторная кора
- Yong-Xin Shi et al, 1998 - Мышцы верхних дыхательных путей
- Zimmermann, 1980 - Динамика артикуляции
- Zocchi et al, 1990 - Дыхательные мышцы